


Using “Food Is Medicine” to Invest in a Healthier America
Highlights from Senator Bill Frist, MD's Congressional Testimony

Last fall, I testified in Congress about the health benefits of “Food is Medicine,” an approach that integrates food-based nutrition interventions into healthcare to address specific health needs and recognizes the sizable role food plays in long-term health outcomes. This strategy treats nutritious food as both preventive care and medical therapy for conditions like diabetes, pregnancy complications, heart failure, chronic kidney disease, and cancer.
With the “Make America Healthy Again” movement gaining steam at the highest levels of our government, implementing strategies that allow nutritious food to finally be included as an essential part of health and healthcare will be vital to moving the needle on our nation’s burgeoning health care costs, obesity rates, and rates of chronic disease. I detail below why this action is needed now, and the data that makes clear why it works. Read my full written testimony for recommendations to Congress on how we get there.
Summary & Excerpts from my testimony before the U.S. House Committee on Ways and Means, Subcommittee on Health on September 18, 2024:
Dear Chairman Buchanan, Ranking Member Doggett, and distinguished members of the Committee:
I am grateful for the opportunity to testify and share what I have seen and learned about food and health as a heart and lung transplant surgeon, as the former Majority Leader of the U.S. Senate, and as a Senior Fellow at the Bipartisan Policy Center, including co-chairing the BPC’s Food is Medicine Working Group.
I’ve personally performed many hundreds of heart surgeries, and written thousands of prescriptions, for patients to treat and prevent disease. But in all my years of practice, I never wrote a prescription for food. That is about to change. Why? Because nutritious food is finally being recognized as a fundamental component of health and health care.

WHERE WE ARE TODAY
Key point #1: Poor nutrition is the leading risk factor for death and disability in the United States, causing more health harms than other major risk factors such as tobacco use, alcohol, opioids, physical inactivity, or air pollution (Figure 1).[1]
Poor diets are estimated to kill 10,000 Americans each week, cause 1,500 new cases of cancer each week, and cause 16,000 new cases of diabetes each week.[2],[3],[4]
Poor diets are a key contributor to 7 in 10 adults being overweight or having obesity,[5] 1 in 2 having diabetes or prediabetes,[6] and 14 in 15 (~93%) having suboptimal cardiometabolic health (less than suboptimal levels of body fat, blood pressure, blood cholesterol, or blood sugar).[7]
Children and teenagers aren’t spared—among 2-5 year-olds, 1 in 8 has obesity. Among teens, 1 in 4 has obesity,[8] and nearly 1 in 3 has prediabetes.[9]

Key Point #2: Poor nutrition is crushing our economy. The U.S. economy loses an estimated $1.1 trillion each year in direct medical costs and productivity losses due to poor nutrition.[10]
For just one condition, type 2 diabetes – a malady almost entirely preventable and treatable with good nutrition – the U.S. government spends nearly $200 billion each year on direct medical costs alone.[11] This is more than the entire budgets of many agencies.
If Congress wants to do the things that you believe are important for the American people, we will never have the funds you need until we reduce healthcare spending. And healthcare spending will never be controlled until we fix food.
Key Point #3: This is also an urgent matter of national security.8 Mission:Readiness, a group of more than 700 retired U.S. generals and admirals, have been making this case for more than a decade.
Today, nearly 8 in 10 young Americans do not quality for military service, and the top medical disqualifier is overweight and obesity.
Key Point #4: The burdens of our food are also driving societal discord. Americans of all incomes, races, and ethnicities —and all political parties, states, and cites — are experiencing high and rising levels of diet-related diseases and downstream family, community, and economic consequences. But those with lower incomes, living in rural communities and from historically marginalized racial and ethnic groups face the greatest burdens.[12]
44 million Americans — about 1 in 8 households — experience food insecurity at some point during the year.[13] Food insecurity is associated with worse nutrition, higher rates of diet-related diseases, and greater healthcare spending.
THE POWER OF “FOOD IS MEDICINE”
"Food is Medicine" (FIM) integrates food-based nutrition interventions into healthcare to address specific health needs and promote health equity. This strategy treats nutritious food as both preventive care and medical therapy for conditions like diabetes, pregnancy complications, heart failure, chronic kidney disease, and cancer.
FIM functions as a medical therapy that simultaneously addresses social determinants of health like food insecurity and poverty—making it a "double duty" intervention gives all Americans fair opportunities to achieve optimal health.
Key components of FIM programs include:
Physician screening for medical conditions and social needs
Insurance-covered food interventions (medically tailored meals, groceries, or produce prescriptions)
Nutrition coaching and culinary education from Registered Dietitian Nutritionists
Supporting elements crucial to FIM's success:
Integration with electronic medical records and clinical pathways
Medical nutrition education for healthcare providers
Partnerships with community organizations to facilitate enrollment in federal assistance programs
Research evaluating outcomes and effectiveness across populations
By providing meals, groceries, or produce through healthcare channels, FIM effectively treats diet-sensitive conditions while overcoming barriers of cost, transportation, and nutritional knowledge—creating a comprehensive approach that is both effective and cost-efficient.
What evidence do we have to back it up?
Research conducted by experts around the country shows that FIM programs work to improve physical health by increasing intake of healthy foods, reducing food insecurity, and improving health outcomes.
Observed benefits include lower hemoglobin A1c (a measure of average blood sugar levels over a 3-month period), body mass index, and blood pressure, as well as improved mental health and disease self-management.
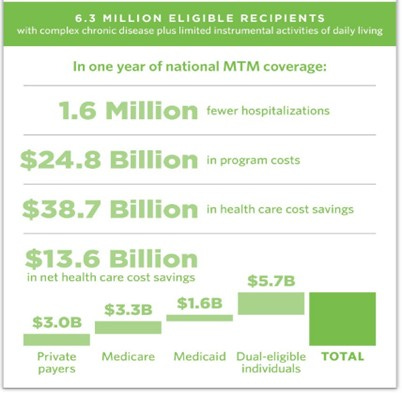
For high-risk patients with complex medical conditions, FIM programs are cost-effective or cost-saving compared to many standard medical interventions. With 1% of Americans generating 25% of healthcare costs and 5% generating 50%, these high-risk patients are ideal candidates for FIM interventions:
Tufts University research found medically tailored meals created net annual savings of $9,000 per patient
Providing medically tailored meals to approximately 6 million qualifying Americans could save nearly $14 billion annually
Medical groceries and produce prescriptions show similar cost benefits
North Carolina's Medicaid waiver program with FIM components delivered to 20,000 beneficiaries across 33 counties resulted in net cost savings
Tufts University estimates that $45 monthly produce prescriptions for Americans with diabetes and food insecurity would prevent 65,000 cardiovascular events within 5 years at no additional net cost, and prevent nearly 300,000 cardiovascular events while saving over $3 billion over a lifetime
Additionally, FIM programs support local food systems, farmers, and rural communities. Programs like Recipe4Health in Alameda County, California prioritize procurement from local small and mid-sized farmers, creating economic benefits for agricultural communities.
It’s time for Congressional action to bring FIM to the American people.
Read the full written testimony here.
[1] U.S. Burden of Disease Collaborators, Mokdad AH, Ballestros K, et al. The State of US Health, 1990-2016: Burden of Diseases, Injuries, and Risk Factors Among US States. JAMA. 2018;319(14):1444-1472. https://jamanetwork.com/journals/jama/fullarticle/2678018
[2] Ibid.
[3] Zhang FF, Cudhea F, Shan Z, et al. Preventable Cancer Burden Associated With Poor Diet in the United States. JNCI Cancer Spectr. 2019;3(2):pkz034. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6649723/
[4] O'Hearn M, Lara-Castor L, Cudhea F, et al. Incident type 2 diabetes attributable to suboptimal diet in 184 countries. Nature medicine. 2023;29(4):982-995. https://www.nature.com/articles/s41591-023-02278-8
[5] https://www.cdc.gov/nchs/fastats/obesity-overweight.htm Accessed September 1, 2024.
[6] CDC. National Diabetes Statistics Report 2024. https://www.cdc.gov/diabetes/php/data-research/index.html
[7] O’Hearn et al. JACC. 2022 Jul, 80 (2) 138–151. https://www.jacc.org/doi/10.1016/j.jacc.2022.04.046
[8] https://www.cdc.gov/obesity/php/data-research/childhood-obesity-facts.html Accessed September 1, 2024.
[9] Liu et al., 2022. JAMA Pediatrics. https://jamanetwork.com/journals/jamapediatrics/fullarticle/2790364
[10] The Rockefeller Foundation. True Cost of Food: Measuring What Maters to Transform the U.S. Food System. 2021. htps://www.rockefellerfoundaon.org/report/true-cost-of-food-measuring-what-maters-to-transform-the-u-s-food-system/.
[11] Parker ED, Lin J, Mahoney T, et al. Economic Costs of Diabetes in the U.S. in 2022. Diabetes Care. 2024;47(1):26-43. https://pubmed.ncbi.nlm.nih.gov/37909353/
[12] Benavidez et al. 2024. Preventing Chronic Disease. https://www.cdc.gov/pcd/issues/2024/23_0267.htm
[13] https://www.ers.usda.gov/topics/food-nutrition-assistance/food-security-in-the-u-s/key-statistics-graphics/
This email was sent to "askusda.gov" on March 22, but sadly, no one has followed up.
Good Afternoon,
President Trump's pick for the new FDA Commissioner, Marty Makary, has identified the root causes why Americans are the most overmedicated and sickest population in the world, because he said, "We have poisoned our food supply."
I believe Makary is aware of the "whitewashing" the previous FDA has perpetrated upon the American people.
For example, the FDA's website (www.fda.gov), dated July 2024, makes the claim even today by answering the question, "Are GMO foods on the market safe to eat?" FDA's answer is "Yes. GMO foods are carefully studied before they are sold to the public to ensure they are as safe as the foods we currently eat. These studies show that GMOs do not affect you differently than non-GMO foods."
I note that the FDA has zero peer-review studies on Americans consuming GMO foods, but their studies are all about the economic benefits of producing and harvesting GMO crops as well as yields and other scientific reports and studies and have nothing to do with the American people eating GMO food and the health-related risks.
The 2020 to 2025 Dietary Guidelines for Americans makes no mention of any unhealthy food to avoid; at the same time, it is very aware of all the chronic diseases putting forward their expert advice, that Americans, by, "Establishing and maintaining a healthy dietary pattern can help minimize diet-related chronic disease risk."
This sounds more like a disclaimer by the USDA and HHS Departments because they know the truth, that GMO foods which makes up, at least 75% of everything in the food store, is what's causing the chronic diseases, already tested by actual MD family doctors' patients with entire families, comparing "Organic food" diets and witnessing first the chronic diseases all going away, and the family becoming healthy again!
My question is, given the new FDA Commissioner's knowledge of the problem, and enforcing for the first time food safety laws that require labelling of GMO foods, and other regulated chemical food additives known to increase chronic disease risks,
What are the provisions the USDA is putting in place now to fill the shortage of "healthy food options" similar to organic foods without the high cost to the American family? Is a New Budget planned for this potential army of Agrarian farmers to fill this shortfall? Spring is almost here?
Thank you for your consideration.
Quentin
Silver sneakers is indeed a great program, but what I'm seeing in my own practice, doing homecare, is a lot of patients have lost the ability to drive.
I have often thought that once the school buses drop the kids off to school, that may be some of the specialized buses could round on the older community, and bring them to the healthcare campus for water aerobics?
Not only is this physical activity excellent for them, to prevent falls and further complications due to heart, disease and diabetes, but it also provides socialization for the elderly.
Much of what I see, daily, is that these patients return home, after acute hospitalization and rehab, only to lounge once again in their La-Z-Boy recliners, watching the news, and big Pharma commercials.